Ovulation Calculator for Irregular Periods and PCOS
Free Ovulation Calculator 2026 — predict your ovulation date, fertile window, and conception probability. Medically reviewed. PCOS-friendly. 100% private.
Normal range: 21–35 days
Typical range: 12–16 days
Health & Fitness Calculators
Track your health and fitness goals.
📖 How to Use the Ovulation Calculator
- 1. Enter the first day of your last period
Select the first day of bleeding from your most recent menstrual period using the date picker.
- 2. Enter your average cycle length
Input the length of your typical cycle (usually 21–35 days; 28 days is average).
- 3. Optionally adjust your luteal phase
Adjust only if you have tracked your personal luteal phase using BBT.
- 4. Click Calculate
Instantly see your predicted ovulation date, fertile window, and next period date.
- 5. Review conception probability by fertile day
Check the chart showing pregnancy probability for each day of your fertile window.
- 6. Combine with physical fertility signs
Track cervical mucus, basal body temperature, or use an OPK to confirm ovulation.
Ovulation Calculation Formula
Ovulation Date = First Day of Last Period + (Cycle Length − Luteal Phase Length)Fertile Window Start = Ovulation Date − 5 daysFertile Window End = Ovulation Date + 1 dayNext Period Date = First Day of Last Period + Cycle LengthCurrent Cycle Day = Days Since Last Period + 1Example (28-day cycle, 14-day luteal phase)
Ovulation = Last Period + (28 − 14) = Day 14 Fertile Window = Day 9 → Day 15
✨ Key Features of the Ovulation Calculator
- Ovulation date prediction
- 6-day fertile window calculation
- Research-based conception probability by day
- Dynamic cycle phase distribution chart
- Today's fertility likelihood indicator
- PCOS and irregular cycle guidance
- Anovulation warning signs
- Cervical mucus fertility guide
- Male factor fertility optimization
- Implantation window tracker
- When to see a fertility specialist guidance
- Downloadable fertility optimization checklist
- Privacy-first — no data stored or transmitted
Ovulation is the process of your ovary releasing a mature egg into the fallopian tube. This is the critical event that makes pregnancy possible. For conception to occur, a sperm must fertilize the egg during its viable window, which is typically 12 to 24 hours after ovulation.
While the egg remains viable for only about a day, sperm can survive in the female reproductive tract for up to five days under ideal conditions. This is why your fertile window extends several days before ovulation — intercourse during the days leading up to ovulation significantly increases the chances of pregnancy because sperm can be present and waiting when the egg is released.
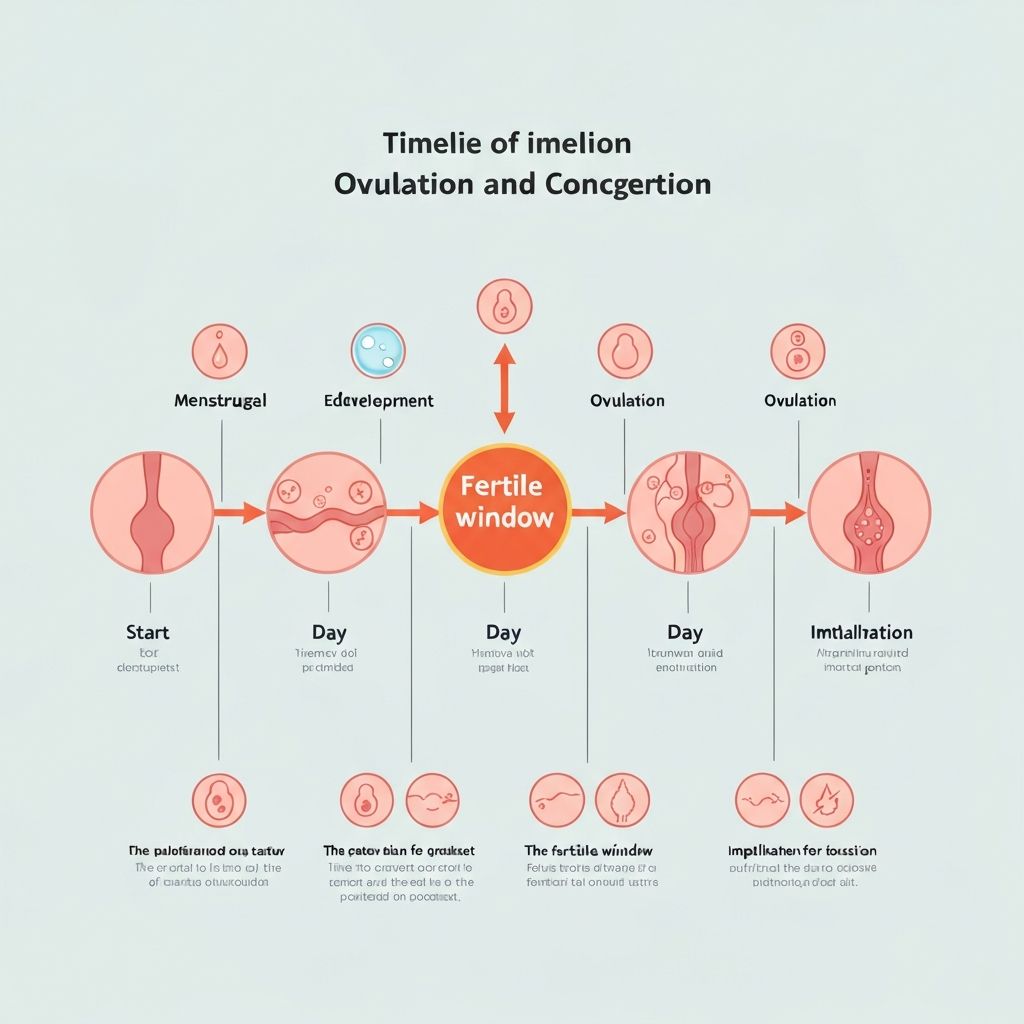
Timeline illustrating the ovulation process, sperm lifespan, egg viability, and the resulting fertile window for conception.
Irregular menstrual cycles present a significant challenge for fertility prediction because the timing of ovulation becomes less predictable. When cycle lengths vary considerably from month to month, predicting your fertile window based on average calculations becomes less reliable.
If you experience irregular periods, consider tracking multiple fertility signs in addition to calendar-based predictions. These signs include changes in cervical mucus consistency (described in detail below), shifts in basal body temperature, and physical sensations like minor cramping or breast tenderness. Ovulation predictor kits can also help confirm ovulation timing more reliably.
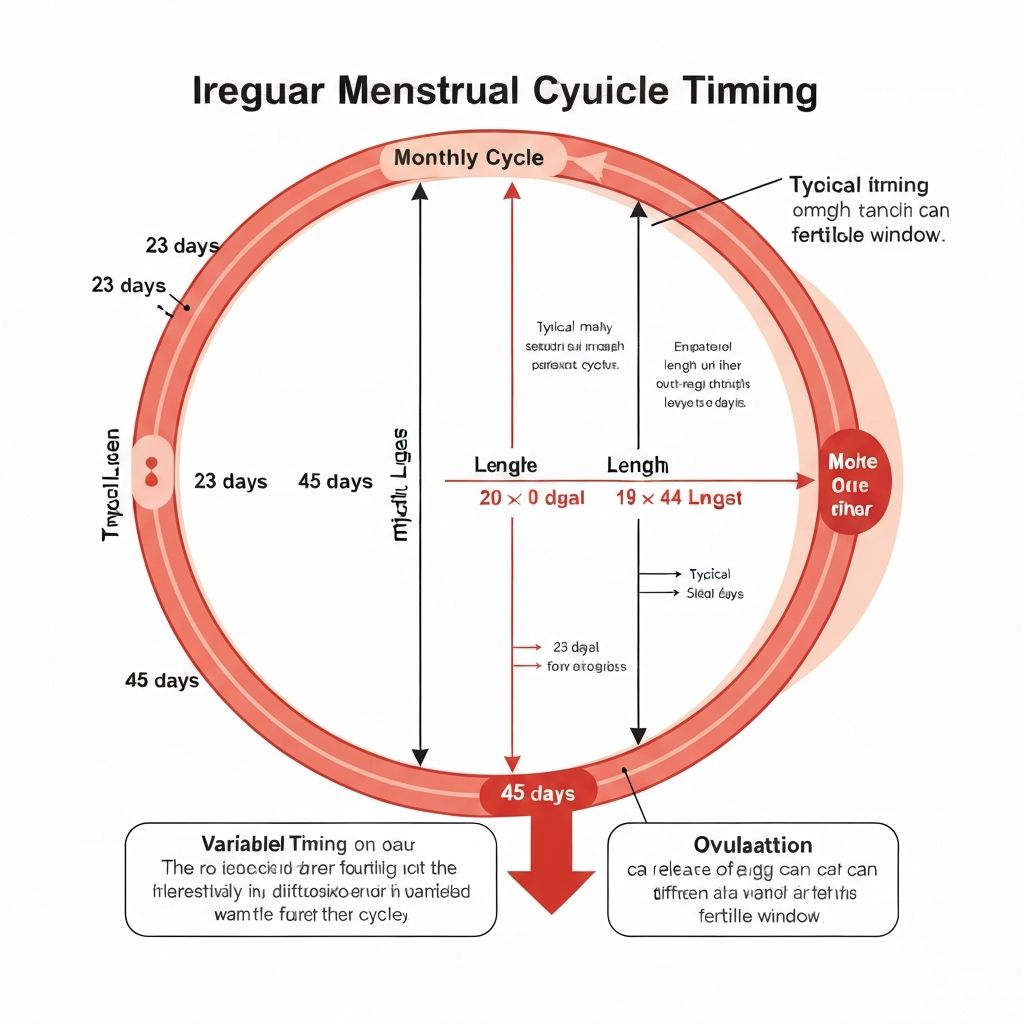
Illustration demonstrating how cycle length variability affects ovulation timing in irregular menstrual cycles.
Polycystic ovary syndrome (PCOS) affects an estimated 8–13% of reproductive-age women and is the leading cause of anovulation — cycles in which no egg is released. Because standard calendar-based calculators assume ovulation occurs at a predictable point in the cycle, they are often less accurate for women with PCOS.
Why PCOS Disrupts Ovulation Timing
In PCOS, elevated androgens (testosterone) and disrupted LH-to-FSH ratios (often 2:1 or 3:1 instead of the normal 1:1) interfere with follicular development. Follicles begin developing but frequently fail to mature fully and rupture to release an egg. This results in cycle lengths ranging from 21 to 90+ days, making calendar prediction unreliable.
More Reliable Tracking Methods for PCOS
Digital OPKs (not strip tests)
Women with PCOS often have chronically elevated LH, which causes false positives on strip OPKs. Digital OPKs that identify the LH surge pattern relative to your personal baseline are more reliable.
Basal Body Temperature (BBT)
A confirmed temperature rise of 0.3–0.5°F maintained for 3+ days after a potential ovulation date is the only way to retrospectively confirm ovulation occurred.
Cervical mucus monitoring
Egg-white cervical mucus (clear, stretchy, 5–10 cm) is a reliable physical sign of impending ovulation even in irregular cycles. It typically appears 1–3 days before ovulation.
Transvaginal ultrasound
For medically supervised cycles, ultrasound monitoring of follicle growth is the gold standard for confirming ovulation timing in PCOS. Discuss this with your OB-GYN or fertility specialist.
Evidence note: Inositol supplementation (myo-inositol 2–4 g/day, or myo:D-chiro ratio 40:1) has emerging research support for restoring ovulatory frequency in PCOS. Discuss with your doctor before starting any supplement protocol.
Anovulation — a menstrual cycle in which no egg is released — can occur even when bleeding happens. A period-like withdrawal bleed can occur without ovulation when progesterone drops, which can be misleading. You may be having cycles without realizing you are not ovulating.
Warning Signs That You May Not Be Ovulating
Cycles consistently shorter than 21 days or longer than 35 days
No basal body temperature rise despite 3+ months of consistent daily tracking
Ovulation predictor kits remain consistently negative throughout the cycle
Absent or very light periods (< 2 days, very light flow)
No change in cervical mucus throughout the cycle — always dry or always sticky
Significant weight change (over- or under-weight) accompanied by cycle irregularity
History of excessive exercise or low body fat (athletes, dancers)
High stress, major life events, or recent illness preceding irregular cycles
When to seek medical evaluation: If you have two or more of the warning signs above, or if you have been trying to conceive for 6–12 months without success, consult a gynecologist. Blood tests (Day 3 FSH/LH/estradiol, Day 21 progesterone, AMH) and a pelvic ultrasound can assess ovarian function. Anovulation is treatable — common causes include PCOS, thyroid disorders, hyperprolactinemia, and low body weight, most of which respond well to treatment.
Your menstrual cycle is divided into four distinct phases, each with its own hormonal patterns and body changes. Understanding these phases helps you recognize your body's natural rhythm and better predict your fertile window.
Menstrual Phase (Days 1–5)
Your uterine lining sheds through your cervix and vagina. This phase typically lasts 3 to 7 days and marks the beginning of your cycle. FSH begins rising to stimulate new follicle development.
Follicular Phase (Days 1–13)
Your body releases follicle-stimulating hormone (FSH), causing your ovaries to develop follicles containing eggs. Estrogen levels rise as follicles grow, thickening your uterine lining and improving cervical mucus quality.
Ovulation Phase (Day 14)
A surge in luteinizing hormone (LH) triggers your ovary to release the mature egg. This is the most fertile time of your cycle. The LH surge peaks 10–12 hours before ovulation and is detectable by OPKs 24–36 hours before egg release.
Luteal Phase (Days 15–28)
The ruptured follicle becomes the corpus luteum, which secretes progesterone to prepare the uterine lining for implantation. If fertilization does not occur, the corpus luteum degenerates, progesterone drops, and menstruation begins. The luteal phase is the most consistent phase across cycles (typically 12–16 days).
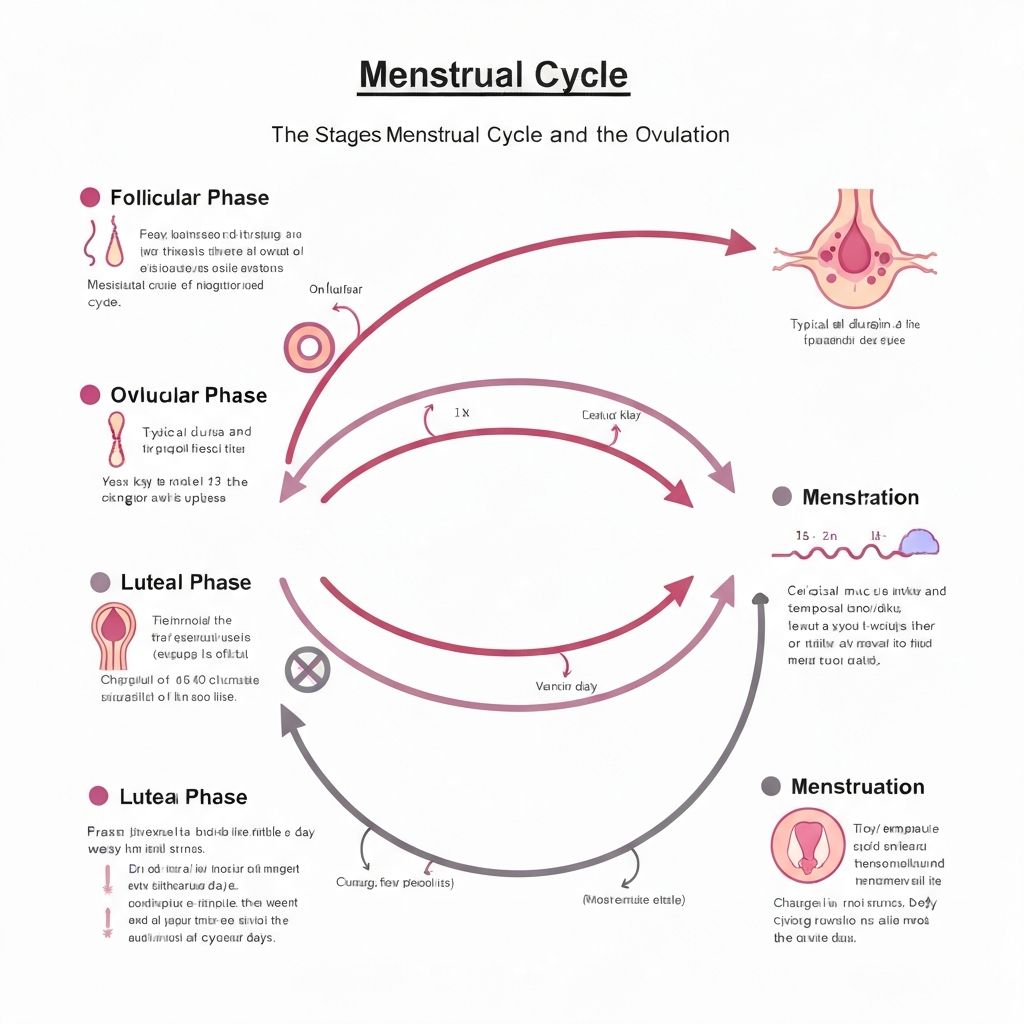
Comprehensive diagram showing all four menstrual cycle phases, hormone levels, and their relationship to ovulation.
Basal body temperature (BBT) is your lowest body temperature, measured immediately upon waking before any physical activity. Tracking BBT over several cycles can help you identify your ovulation pattern. During the follicular phase and before ovulation, your temperature typically remains around 96.4°F to 96.8°F (35.8°C to 36°C).
After ovulation, progesterone secreted by the corpus luteum causes a slight temperature rise of 0.3°F to 0.5°F (0.2°C to 0.3°C), which persists until your period begins. BBT tracking confirms ovulation in retrospect rather than predicting it in advance — you will see the temperature rise the day after ovulation has occurred. Combining BBT with cervical mucus observation and OPK testing provides the most comprehensive picture of your fertility.
BBT accuracy tips: Take your temperature at the same time every morning (±30 minutes), using the same thermometer, before getting out of bed, drinking, or speaking. Illness, alcohol, travel across time zones, and poor sleep (<4 hours) can artificially raise BBT. Mark these disruptions on your chart so you can interpret the pattern accurately.
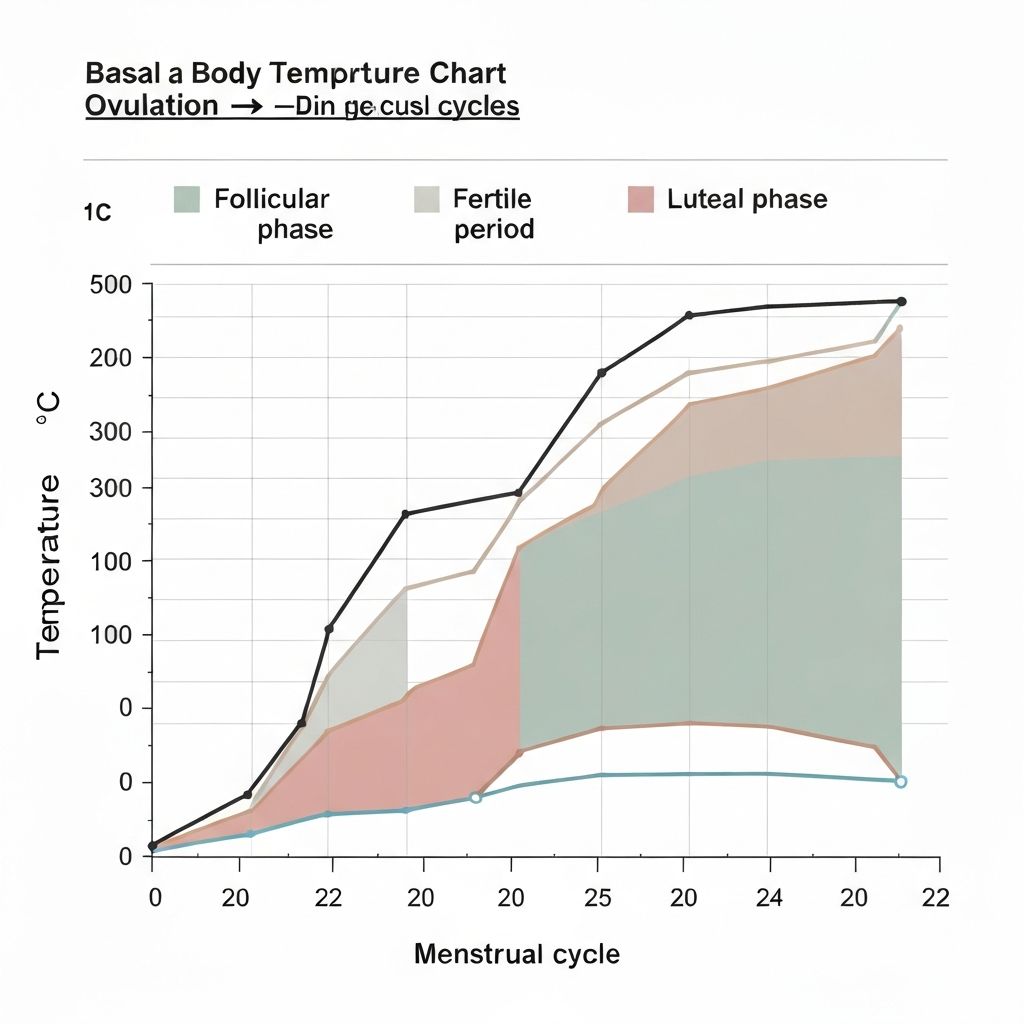
Sample BBT chart illustrating the temperature dip before ovulation and the post-ovulation temperature rise.
Your body provides several physical and hormonal signs that ovulation is occurring or about to occur. Recognizing these signs helps you time intercourse for maximum fertility when combined with calculator predictions.
Ovulation Predictor Kits (OPKs): Detecting the LH Surge
Ovulation predictor kits (OPKs) detect the surge in luteinizing hormone (LH) that triggers ovulation. A positive result typically indicates ovulation will occur within 24 to 36 hours. For best results, begin testing about 17 days before your expected period and test at the same time each day (afternoon is optimal — LH surges in the morning but takes several hours to appear in urine).
Important for PCOS: Women with PCOS may have chronically elevated LH, causing strip OPKs to show a faint positive throughout the cycle. Digital OPKs that measure your personal LH baseline are more reliable in this case.

OPK test strip demonstrating positive result indicating LH surge.
How Can I Increase My Chances of Getting Pregnant?
Beyond timing intercourse during your fertile window, several lifestyle factors support your fertility goals.
- •Time intercourse properly: Focus on the 2–3 days before ovulation — the highest probability window per research data.
- •Maintain a balanced diet: Include folate (400–800 mcg daily), iron, antioxidants, and omega-3 fatty acids.
- •Exercise moderately: 30 minutes, 5x per week. Avoid over-exercising (> 60 min/day strenuous) which can suppress ovulation.
- •Manage stress: Cortisol directly suppresses GnRH — practice mindfulness, yoga, or therapy if TTC stress is significant.
- •Optimize sleep: 7–9 hours nightly. Circadian disruption (shift work, chronic poor sleep) affects reproductive hormone cycles.

Healthy lifestyle practices that support fertility and reproductive health.
Cervical mucus (CM) is produced by glands in the cervix and changes in texture, color, and quantity throughout your cycle in direct response to estrogen and progesterone. Learning to read your cervical mucus is one of the most reliable — and completely free — ways to identify approaching ovulation.
| Cycle Phase | Mucus Type | Appearance & Sensation | Fertility |
|---|---|---|---|
| Post-period (Days 4–6) | Dry | No visible mucus, dry sensation | Not fertile |
| Early follicular (Days 7–9) | Sticky | White or yellow, sticky, crumbly — like paste | Low fertility |
| Mid-follicular (Days 10–12) | Creamy | White or cream, lotion-like, smooth — does not stretch | Some fertility |
| Peak fertility (Days 13–15) | Egg-white (EWCM) | Clear, slippery, stretchy 5–10 cm — like raw egg white. Very wet sensation. | Peak fertility ★ |
| Post-ovulation (Days 16+) | Sticky → Dry | Returns to sticky or dry as progesterone rises | Not fertile |
Practical tip: Check cervical mucus every time you use the bathroom by wiping with dry toilet paper before urinating, or by collecting a small amount with clean fingers. Record the observation daily. Egg-white cervical mucus (EWCM) is your most reliable advance signal of ovulation — when you see it, ovulation is typically 1–3 days away.
Male factor infertility contributes to approximately 40–50% of all infertility cases, yet most ovulation calculator resources focus entirely on the female cycle. Optimizing sperm health during the 74-day sperm maturation cycle (spermatogenesis) significantly improves conception outcomes when timed with your fertile window.
Timing and frequency
- •Have intercourse every 1–2 days during the fertile window — daily is not superior to every other day and may cause anxiety
- •Abstaining for more than 4–5 days before the fertile window reduces sperm motility
- •Sperm takes 64–74 days to mature — lifestyle changes take ~3 months to improve sperm parameters
Temperature and lifestyle
- •Avoid hot baths, saunas, and hot tubs — testicular temperature must stay 2–4°C below core body temperature for optimal sperm production
- •Avoid tight underwear and prolonged laptop use on the lap
- •Quit smoking — tobacco reduces sperm count, motility, and DNA integrity significantly
Nutrition and supplements
- •Zinc (11 mg/day) and selenium (55 mcg/day) are critical for testosterone production and sperm motility
- •Coenzyme Q10 (200–600 mg/day) improves sperm motility — backed by randomised controlled trial evidence
- •Folate (400 mcg/day) and vitamin D reduce sperm DNA fragmentation
- •Limit alcohol to <5 units/week; avoid recreational drugs entirely
When to seek a semen analysis
- •After 6–12 months TTC, request a semen analysis — it is non-invasive, quick, and often the first diagnostic test offered
- •Normal parameters: count >16 million/ml, motility >42%, morphology >4% normal forms (WHO 2021 criteria)
- •A single abnormal semen analysis is not diagnostic — values fluctuate based on illness, stress, and abstinence period
If fertilization occurs, the fertilized egg (zygote) travels through the fallopian tube over 5–7 days, dividing and developing into a blastocyst. The blastocyst implants into the uterine lining during the implantation window — a hormonally controlled period when the endometrium is receptive to the embryo.
Egg released. LH surge peaked 24–36 hours before. Egg viable for 12–24 hours.
Fertilization occurs in the fallopian tube (if sperm present). Zygote begins dividing, developing into a morula then blastocyst.
Implantation window. Blastocyst reaches the uterus and embeds into the endometrium. hCG production begins after successful implantation.
Some women experience implantation spotting — light pink or brown discharge for 1–3 days. Not experienced by all women.
hCG levels rise enough for early detection pregnancy tests. Wait until Day 14 (missed period) for most accurate result.
When to take a pregnancy test: For the most reliable result, test on the first day of your missed period (approximately 14 days after ovulation). Testing earlier risks a false negative — hCG may not yet be high enough to detect, even if implantation has occurred. hCG doubles every 48–72 hours in the first weeks of pregnancy.
Ovulation calculators and cycle tracking are valuable first steps, but some situations warrant prompt medical evaluation. The following evidence-based guidelines (per ACOG and RCOG recommendations) will help you know when it's time to consult a reproductive endocrinologist or fertility-specialized OB-GYN.
Under 35
After 12 months of regular (every 2–3 days) unprotected intercourse without conception
Ages 35–39
After 6 months of regular unprotected intercourse without conception
Over 40
After 3 months — or consult immediately to discuss options proactively
Seek evaluation sooner, regardless of age, if you have:
Irregular, infrequent, or absent periods
Known or suspected PCOS, endometriosis, or uterine fibroids
Two or more consecutive pregnancy losses
A history of pelvic inflammatory disease (PID)
Cancer treatment history (chemotherapy or radiation)
A partner with a known or suspected fertility issue
Very painful periods (potential endometriosis)
Previous ectopic pregnancy or tubal surgery
First appointment checklist: Bring 3–6 months of cycle tracking data (BBT charts, OPK results, cycle lengths), a list of current medications and supplements, and details of any previous pregnancies. Your doctor will likely order bloodwork (FSH, LH, AMH, estradiol, thyroid, prolactin) and a pelvic ultrasound as initial investigations.
Privacy Guarantee
All calculations are performed locally in your browser. No personal health data is ever transmitted to any server or third party. Your cycle history is stored only in your own browser's local storage and is automatically cleared after 3 days.
Dr. Emily Carter, MD
Board-Certified Obstetrician & Gynecologist
Women's Health & Reproductive Medicine · Last reviewed: December 2025
Review scope: Fertility calculation methodology, cycle phase science, ovulation timing accuracy, PCOS-specific guidance, anovulation criteria, and implantation window timing have been reviewed for informational accuracy against current clinical evidence.
Limitations: This calculator provides estimates based on average cycle patterns. Individual ovulation timing varies due to hormonal fluctuations, stress, illness, age, and underlying conditions. Results do not replace medical advice or professional fertility evaluation.
Important: If you have irregular cycles, PCOS, endometriosis, recurrent miscarriage, or any condition affecting reproduction, consult a qualified healthcare provider for personalised guidance. This tool is for educational and informational purposes only.
Scientific References & Sources
- 1.Wilcox AJ, Weinberg CR, Baird DD. Timing of sexual intercourse in relation to ovulation — effects on the probability of conception, survival of the pregnancy, and sex of the baby. N Engl J Med. 1995;333(23):1517–1521. pubmed.ncbi.nlm.nih.gov/7477165
- 2.Dunson DB, Colombo B, Baird DD. Changes with age in the level and duration of fertility in the menstrual cycle. Hum Reprod. 2002;17(5):1399–1403. pubmed.ncbi.nlm.nih.gov/11980771
- 3.World Health Organization. Infertility — Key Facts. WHO, 2023. who.int/news-room/fact-sheets/detail/infertility
- 4.National Institute of Child Health and Human Development (NICHD). Polycystic Ovary Syndrome (PCOS) — Condition Information. NIH, 2021. nichd.nih.gov/health/topics/pcos/conditioninfo
- 5.American College of Obstetricians and Gynecologists (ACOG). Evaluating Infertility — FAQs. ACOG, 2022. acog.org/womens-health/faqs/evaluating-infertility
- 6.U.S. National Library of Medicine — MedlinePlus. Ovulation. NIH MedlinePlus, 2023. medlineplus.gov/ovulation.html
- 7.Gurner KL, Bhatt S. Anovulation — StatPearls. NCBI Bookshelf, NIH, 2023. ncbi.nlm.nih.gov/books/NBK279054
- 8.Su HW, Yi YC, Wei TY, Chang TC, Cheng CM. Detection of ovulation, a review of currently available methods. Bioeng Transl Med. 2017;2(3):238–246. pubmed.ncbi.nlm.nih.gov/29313033
Content on this page is for informational purposes only and is reviewed against peer-reviewed literature and guidelines from established medical organisations. Always consult a qualified healthcare provider for personalised medical advice.
How do I calculate my ovulation day?
Subtract your luteal phase length (typically 14 days) from your total cycle length. For a 28-day cycle: 28 − 14 = Day 14 from the start of your period. Our calculator performs this automatically. For irregular cycles, use the average of your last 3–6 cycles as your cycle length input.
What is the fertile window?
The fertile window is the 6-day period when conception is possible: the 5 days before ovulation plus ovulation day itself. Sperm can survive in the female reproductive tract for up to 5 days, while the egg is viable for only 12–24 hours after ovulation. The 2–3 days before ovulation carry the highest conception probability (up to 31%, per Wilcox et al., 1995).
Can you ovulate with irregular periods or PCOS?
Yes, but timing is unpredictable. Women with PCOS may experience anovulatory cycles. Track basal body temperature (for a post-ovulation rise of 0.3–0.5°F), egg-white cervical mucus, and use a digital OPK. Calendar-only prediction is unreliable for cycles varying by more than 7 days.
What are the signs of ovulation?
Key signs include: egg-white cervical mucus (clear, stretchy, 5–10 cm), a 0.3–0.5°F rise in basal body temperature the morning after ovulation, a positive OPK (LH surge), mild one-sided pelvic pain (Mittelschmerz), breast tenderness, and increased libido. Combining multiple signs gives the most reliable prediction.
Can stress delay ovulation?
Yes. Chronic stress elevates cortisol, which suppresses GnRH from the hypothalamus, disrupting the FSH and LH hormonal cascade required to trigger ovulation. This can delay ovulation by several days or cause complete anovulation in a cycle. Calendar predictions based on past cycle lengths may be inaccurate during highly stressful periods.
What is anovulation and how do I know if I have it?
Anovulation is the absence of ovulation in a cycle. Signs include: no BBT temperature rise despite tracking, consistently negative OPKs, cycles shorter than 21 or longer than 35 days, very light or absent periods, and no cervical mucus changes. PCOS is the most common cause. Anovulation is confirmed by a Day 21 progesterone blood test below 3 ng/mL, combined with BBT charting.
When should I take a pregnancy test after ovulation?
Wait until 14 days after ovulation — the first day of your missed period — for the most accurate result. Testing earlier risks a false negative. Implantation occurs 6–10 days post-ovulation, and hCG (the hormone tests detect) rises only after implantation. hCG doubles every 48–72 hours in early pregnancy.
When should I see a fertility specialist?
See a fertility specialist after 12 months TTC if under 35, 6 months if aged 35–39, and 3 months (or immediately) if over 40. Seek evaluation sooner if you have irregular periods, PCOS, endometriosis, two or more miscarriages, or a partner with known sperm issues.